Phase I study of BGJ398, a selective pan-FGFR inhibitor in genetically preselected advanced solid tumors
Background: Fibroblast growth factor receptors (FGFRs) play a role in cell proliferation and survival. Genetic alterations of FGFRs can lead to deregulated activation in various cancers, including squamous cell carcinoma (SCC) of the lung and urothelial bladder cancer. Here, we report on a phase I study of BGJ398 a potent, selective pan-FGFR inhibitor.
Methods: Eligible patients (pts; ≥ 18 years of age) had tumors with any FGFR genetic alteration identified by central or local prescreening. Pts received BGJ398 once or twice daily (qd or bid) in 28-day cycles in escalating cohorts. Dose-limiting toxicities (DLTs) were predefined and included both severe events and those resulting in significant dosing delays. Upon determination of maximum tolerated dose (MTD), 3 expansion arms were treated: arm 1 included FGFR1-amplified SCC of the lung (continuous qd dosing); arms 2 and 3 included FGFR-altered solid tumors given qd continuous doses (arm 2) or qd doses on a 3-weeks-on/1-week-off schedule (arm 3).
Results: As of September 24, 2013, 94 pts were enrolled (median age 57.5 years). Pts were treated in qd dose cohorts (5-150 mg; n = 90) or a bid dose cohort (50 mg; n = 4). Arms 1 and 3 are ongoing. Of the 82 pts who discontinued, the most common reasons were disease progression (n = 56), consent withdrawal (n = 12), and adverse events (AEs; n = 10). DLTs during dose escalation were grade 3 aminotransferase increases (1 each at 100 and 125 mg), hyperphosphatemia (125 mg), and grade 1 corneal toxicity (150 mg). The 125-mg qd dose was identified as the MTD. Common treatment-emergent AEs (any grade, suspected to be related) at 125 mg qd (n = 41) include hyperphosphatemia (78%), stomatitis (37%), alopecia (32%), decreased appetite (32%), and fatigue (22%) and were generally mild, with stomatitis (7%) the only grade 3/4 AE occurring ≥ 5%. Elevated serum phosphate levels, a pharmacodynamic marker of FGFR pathway inhibition, could be managed through diet, phosphate lowering therapy, and drug interruptions. Preliminary analysis of efficacy data indicates tumor regressions in pts with various FGFR genetic alterations, including 4 of 5 pts with urothelial cell carcinomas (4 of which originated in the bladder) with FGFR3-activating mutations (with tumor reductions ranging from 27% to 48%). Additionally, 1 pt with FGFR1-amplified SCC lung cancer achieved confirmed partial response (PR) while another pt achieved a PR confirmed after 27 days. Tumor reductions were also observed in cholangiocarcinoma with an FGFR2 gene fusion, and FGFR1-amplified breast cancer.
Conclusions: BGJ398 had a tolerable safety profile and demonstrated single-agent activity in pts with FGFR-genetically altered solid tumors. The 3-weeks-on/1-week-off schedule has been chosen for future studies based on its improved safety profile. Clinical activity was observed in multiple tumor types, and pts with FGFR3-mutated bladder cancer may be especially sensitive to BGJ398. |
 汇总4月最新:临床试验招募| 小细胞
"化疗±免疫后进展了,还能怎么办?"——这是许多小细胞肺癌患者和家属的困境。
临
汇总4月最新:临床试验招募| 小细胞
"化疗±免疫后进展了,还能怎么办?"——这是许多小细胞肺癌患者和家属的困境。
临
 神奇的ommaya囊——学习笔记
一个神奇的装置-ommaya囊——————9.28 苗茜医生科普讲座
直播链接:https://live.
神奇的ommaya囊——学习笔记
一个神奇的装置-ommaya囊——————9.28 苗茜医生科普讲座
直播链接:https://live.
 母亲肺腺癌晚期骨转移,EGFR21突变,
母亲1970年出生,56周岁,身高163cm,体重98kg(196斤)。2025年9月23日肺炎住院,胸
母亲肺腺癌晚期骨转移,EGFR21突变,
母亲1970年出生,56周岁,身高163cm,体重98kg(196斤)。2025年9月23日肺炎住院,胸
 临床试验招募| 铂类化疗失败后的经治
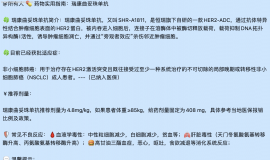
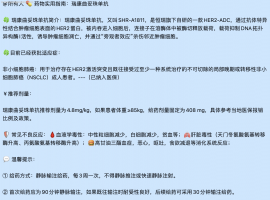
🔥 项目题目:AL8326片治疗至少接受二线治疗方案后疾病进展或复发的小细胞肺癌患者
临床试验招募| 铂类化疗失败后的经治
🔥 项目题目:AL8326片治疗至少接受二线治疗方案后疾病进展或复发的小细胞肺癌患者
 这个春天,我想和你分享!ALK+“从容
作者:pear
宠辱不惊,闲看庭前花开花落;去留无意,漫随天外云卷云舒。
这份古人笔下
这个春天,我想和你分享!ALK+“从容
作者:pear
宠辱不惊,闲看庭前花开花落;去留无意,漫随天外云卷云舒。
这份古人笔下




 显身卡
显身卡